Aravosis: White House: Nearly half the US could get Swine Flu
Kurtz (TPM): Cognitive DissonanceABC:
The report says that under a worst-case scenario, between 60 and 120 million Americans could get sick with the swine flu and another 30 million could contract the virus but not show symptoms. Between 30,000 and 90,000 could die -- more than twice the annual average of deaths associated with the seasonal flu. Those deaths generally occur in people older than 65.
The swine flu is "unusual" however, U.S. Health and Human Services Secretary Kathleen Sebelius said, because it tends to affect children and young adults more harshly than others and "hasn't yet affected seniors."
The report says the skyrocketing infections will peak on Oct. 15 -- the exact date a vaccine is expected to be delivered.
Michael Steele is on Fox now going on about how Medicare is a wreck, completely bankrupt, and an example of how the government has already proven it can't run a health care program.
Except didn't the "health care bill of rights" that the GOP unveiled yesterday declare preserving Medicare and protecting it against any cuts an inviolable right?
Shorter Steele: Medicare is a disaster! Long live Medicare!
(It's not the first time Steele has gotten his Medicare demagoging all messed up.)
Visit msnbc.com for Breaking News, World News, and News about the Economy
Benen: THEY REALLY THINK YOU'RE STUPID....In a sign of real concern about the right wing’s latest lurid health care tale, the Obama administration’s veterans agency is hitting back at conservative media with a detailed factual rebuttal of the claim that government is giving veterans a “death book” that urges them to hurry up and die.
The rebuttal includes a detailed fact sheet and a timeline, both of which were sent my way by an administration official and may be sent widely to reporters later this morning.
Haven’t heard the “death book” tale? It got started with this Op ed piece in The Wall Street Journal by a former Bush official claiming that a manual distibuted by the Department of Veterans Affairs sends veterans a “hurry-up-and-die message.”
The claim — the right’s latest effort to frighten the vulnerable about Obama’s health care intentions — is that the manual steers veterans towards “predetermined concluions” about “end-of-life choices.” It’s gotten tons of right wing and even traditional media play.
The rebuttal points out that the manual, which is called “Your Life, Your Choices,” is not an “advance directive” and “does not promote limitation of life-sustaining treatment, assisted suicide, or euthanasia.” Rather, its goal is to help veterans “consider the types of health care they would want to receive if they were unable to make decisions for themselves” and to “think about and discuss their preferences” with family, friends, and doctors.
The fact sheet does note that the manual was determined under Bush to be in need of revision, and that it may be “too negative in tone and not sufficiently sensitive” to pro-life or disabled veterans. But the rebuttal strongly contests the core “death book” claim, and notes that the author of the original Op ed has offered a competing book, which is for sale.
The Obama administration’s detailed rebuttal is yet another reminder of how aggressively the conservative media is targeting the frail and vulnerable with its outlandish health care tales — so much so that real government resources are required to combat them.
The right's "death panel" attack was thoroughly and completely debunked. It didn't matter -- lots of Americans believed the lie anyway. It has, however, started to lose some of its salience, which means it's time for the new health care reform lie.We talked over the weekend about the "death books" nonsense. The right-wing claim is that the Department of Veterans Affairs is pushing an end-of-life planning document that encourages vets to pursue death. The claim is completely ridiculous.
But it doesn't matter. The disgusting attack worked its way from Fox News to the Wall Street Journal to CNN. Right-wing hacks are pushing this aggressively, and this morning, Republican National Committee Chairman Michael Steele said, "If you want an example of bad public policy, just look at the situation with our veterans when you have a manual out there telling our veterans stuff like 'are you really of value to your community?' You know, encouraging them to commit suicide. I mean, this is crazy coming from the government."
"Crazy" is the operative word here.
We're all accustomed to a certain baseline of dishonesty among opponents of health care reform, but this truly vile. These clowns lost their dignity quite a while ago, but this "death book" stupidity is beneath contempt.
For what it's worth, Olbermann broke down the smear last night, and the Obama administration published a detailed rebuttal to the lurid claim this morning.
Whether the pushback is sufficient remains to be seen. For the right, it's the kitchen-sink strategy -- come up with as many lies as possible, and throw them all at health care reform. When one piece of garbage starts to lose its punch, throw another. Even if it's promptly debunked, plenty of gullible suckers will believe it, and news outlets won't dare say, "Right-wing opponents of reform lie a lot." Indeed, there are no adverse consequences for conservative con artistss at all.
Our political discourse is just so ridiculous, it's sometimes surprising the political system functions at all.
TR Reid: 5 Myths About Health Care Around the World
As Americans search for the cure to what ails our health-care system, we've overlooked an invaluable source of ideas and solutions: the rest of the world. All the other industrialized democracies have faced problems like ours, yet they've found ways to cover everybody -- and still spend far less than we do.
I've traveled the world from Oslo to Osaka to see how other developed democracies provide health care. Instead of dismissing these models as "socialist," we could adapt their solutions to fix our problems. To do that, we first have to dispel a few myths about health care abroad:
1. It's all socialized medicine out there.
Not so. Some countries, such as Britain, New Zealand and Cuba, do provide health care in government hospitals, with the government paying the bills. Others -- for instance, Canada and Taiwan -- rely on private-sector providers, paid for by government-run insurance. But many wealthy countries -- including Germany, the Netherlands, Japan and Switzerland -- provide universal coverage using private doctors, private hospitals and private insurance plans.
In some ways, health care is less "socialized" overseas than in the United States. Almost all Americans sign up for government insurance (Medicare) at age 65. In Germany, Switzerland and the Netherlands, seniors stick with private insurance plans for life. Meanwhile, the U.S. Department of Veterans Affairs is one of the planet's purest examples of government-run health care.
2. Overseas, care is rationed through limited choices or long lines.
Generally, no. Germans can sign up for any of the nation's 200 private health insurance plans -- a broader choice than any American has. If a German doesn't like her insurance company, she can switch to another, with no increase in premium. The Swiss, too, can choose any insurance plan in the country.
In France and Japan, you don't get a choice of insurance provider; you have to use the one designated for your company or your industry. But patients can go to any doctor, any hospital, any traditional healer. There are no U.S.-style limits such as "in-network" lists of doctors or "pre-authorization" for surgery. You pick any doctor, you get treatment -- and insurance has to pay.
Canadians have their choice of providers. In Austria and Germany, if a doctor diagnoses a person as "stressed," medical insurance pays for weekends at a health spa.
As for those notorious waiting lists, some countries are indeed plagued by them. Canada makes patients wait weeks or months for nonemergency care, as a way to keep costs down. But studies by the Commonwealth Fund and others report that many nations -- Germany, Britain, Austria -- outperform the United States on measures such as waiting times for appointments and for elective surgeries.
In Japan, waiting times are so short that most patients don't bother to make an appointment. One Thursday morning in Tokyo, I called the prestigious orthopedic clinic at Keio University Hospital to schedule a consultation about my aching shoulder. "Why don't you just drop by?" the receptionist said. That same afternoon, I was in the surgeon's office. Dr. Nakamichi recommended an operation. "When could we do it?" I asked. The doctor checked his computer and said, "Tomorrow would be pretty difficult. Perhaps some day next week?"
3. Foreign health-care systems are inefficient, bloated bureaucracies.
Much less so than here. It may seem to Americans that U.S.-style free enterprise -- private-sector, for-profit health insurance -- is naturally the most cost-effective way to pay for health care. But in fact, all the other payment systems are more efficient than ours.
U.S. health insurance companies have the highest administrative costs in the world; they spend roughly 20 cents of every dollar for nonmedical costs, such as paperwork, reviewing claims and marketing. France's health insurance industry, in contrast, covers everybody and spends about 4 percent on administration. Canada's universal insurance system, run by government bureaucrats, spends 6 percent on administration. In Taiwan, a leaner version of the Canadian model has administrative costs of 1.5 percent; one year, this figure ballooned to 2 percent, and the opposition parties savaged the government for wasting money.
The world champion at controlling medical costs is Japan, even though its aging population is a profligate consumer of medical care. On average, the Japanese go to the doctor 15 times a year, three times the U.S. rate. They have twice as many MRI scans and X-rays. Quality is high; life expectancy and recovery rates for major diseases are better than in the United States. And yet Japan spends about $3,400 per person annually on health care; the United States spends more than $7,000.
4. Cost controls stifle innovation.
False. The United States is home to groundbreaking medical research, but so are other countries with much lower cost structures. Any American who's had a hip or knee replacement is standing on French innovation. Deep-brain stimulation to treat depression is a Canadian breakthrough. Many of the wonder drugs promoted endlessly on American television, including Viagra, come from British, Swiss or Japanese labs.
Overseas, strict cost controls actually drive innovation. In the United States, an MRI scan of the neck region costs about $1,500. In Japan, the identical scan costs $98. Under the pressure of cost controls, Japanese researchers found ways to perform the same diagnostic technique for one-fifteenth the American price. (And Japanese labs still make a profit.)
5. Health insurance has to be cruel.
Not really. American health insurance companies routinely reject applicants with a "preexisting condition" -- precisely the people most likely to need the insurers' service. They employ armies of adjusters to deny claims. If a customer is hit by a truck and faces big medical bills, the insurer's "rescission department" digs through the records looking for grounds to cancel the policy, often while the victim is still in the hospital. The companies say they have to do this stuff to survive in a tough business.
Foreign health insurance companies, in contrast, must accept all applicants, and they can't cancel as long as you pay your premiums. The plans are required to pay any claim submitted by a doctor or hospital (or health spa), usually within tight time limits. The big Swiss insurer Groupe Mutuel promises to pay all claims within five days. "Our customers love it," the group's chief executive told me. The corollary is that everyone is mandated to buy insurance, to give the plans an adequate pool of rate-payers.
The key difference is that foreign health insurance plans exist only to pay people's medical bills, not to make a profit. The United States is the only developed country that lets insurance companies profit from basic health coverage.
In many ways, foreign health-care models are not really "foreign" to America, because our crazy-quilt health-care system uses elements of all of them. For Native Americans or veterans, we're Britain: The government provides health care, funding it through general taxes, and patients get no bills. For people who get insurance through their jobs, we're Germany: Premiums are split between workers and employers, and private insurance plans pay private doctors and hospitals. For people over 65, we're Canada: Everyone pays premiums for an insurance plan run by the government, and the public plan pays private doctors and hospitals according to a set fee schedule. And for the tens of millions without insurance coverage, we're Burundi or Burma: In the world's poor nations, sick people pay out of pocket for medical care; those who can't pay stay sick or die.
This fragmentation is another reason that we spend more than anybody else and still leave millions without coverage. All the other developed countries have settled on one model for health-care delivery and finance; we've blended them all into a costly, confusing bureaucratic mess.
Which, in turn, punctures the most persistent myth of all: that America has "the finest health care" in the world. We don't. In terms of results, almost all advanced countries have better national health statistics than the United States does. In terms of finance, we force 700,000 Americans into bankruptcy each year because of medical bills. In France, the number of medical bankruptcies is zero. Britain: zero. Japan: zero. Germany: zero.
Given our remarkable medical assets -- the best-educated doctors and nurses, the most advanced hospitals, world-class research -- the United States could be, and should be, the best in the world. To get there, though, we have to be willing to learn some lessons about health-care administration from the other industrialized democracies.
T.R. Reid, a former Washington Post reporter, is the author of "The Healing of America: A Global Quest for Better, Cheaper, and Fairer Health Care," to be published Monday.
DemfromCt (DK): Christopher Hayes Explains Health Reform
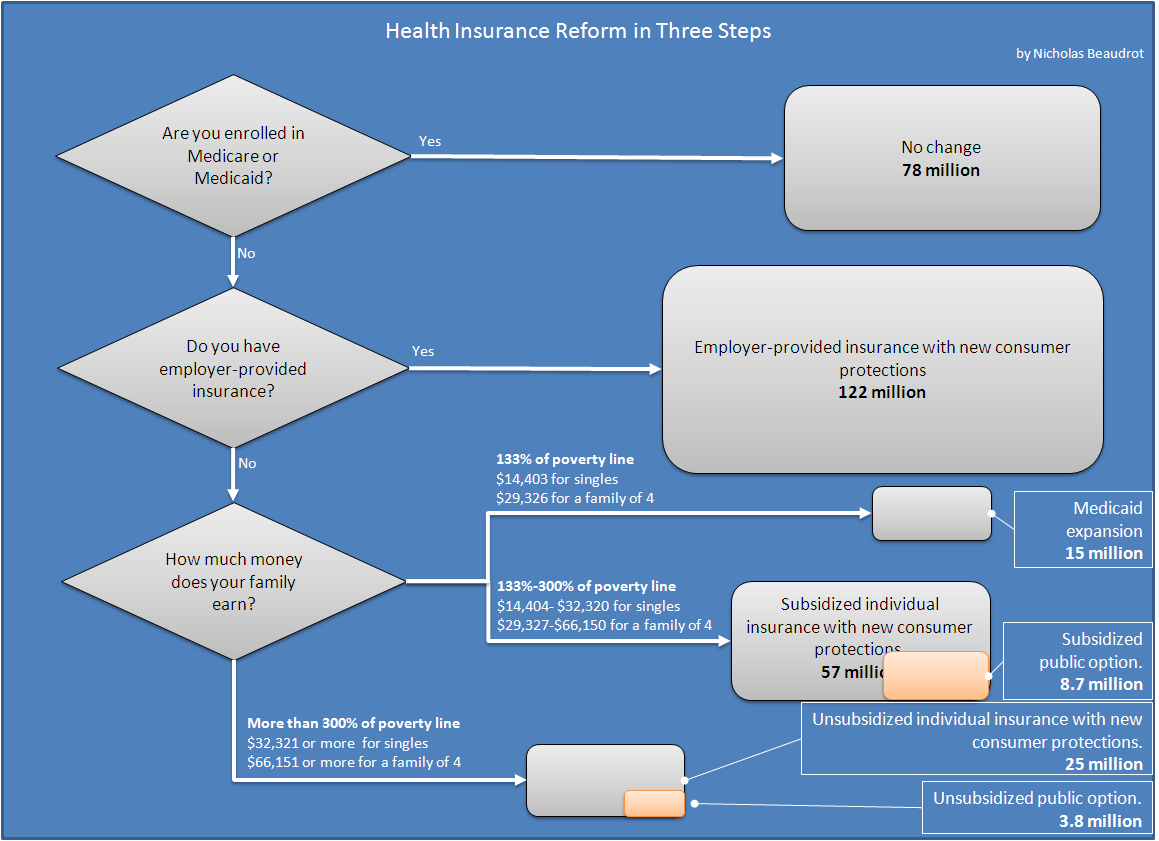
Yglesias: Grassley: Perfection is the StandardAt Netroots Nation, a panel featured Christopher Hayes, Washington DC editor of The Nation, explaining health reform.
Nicholas Beaudrot at Donkeylicious produced this chart (click for readability) to explain it all:
NPR's Richard Knox has his own interactive bit to explain what it means to you.
- ::

In case you were wondering, here’s yet another indication that Chuck Grassley isn’t serious about doing health reform:
“We need to slow down and do a little less,” Mr. Grassley told another town-hall gathering in Pocahontas, Iowa, Monday afternoon. “We need to fix what’s broken and leave alone what’s working well.”
In an interview, he vowed not to vote for an “imperfect bill” that includes a public option or gives the government too much control over end-of-life issues.
It should be obvious that when you’re talking about doing something like comprehensive health care legislation, you’re talking about passing an imperfect bill. Congress just isn’t going to write and pass a perfect bill. The standard is that you try to pass a bill that makes things better. A Senator talking about the need to avoid imperfection is a Senator looking for excuses to vote no. Delaying health reform, meanwhile, is part of an explicit strategy to kill reform. Max Baucus and Barack Obama need to cut this guy loose and drop the “gang of six” nonsense or else it’s very hard to see how anything is possibly going to get done.
No comments:
Post a Comment